We all have fluid chambers in our brain called ventricles. They are filled with a clear fluid called cerebrospinal fluid (CSF).This fluid is very important as it protects and nourishes the brain and the spinal cord. Fluid collection in these spaces usually does not cause a problem.
 However, if these fluid collections exert pressure on the brain and cause symptoms or accelerated head growth, surgical treatment may be required.
However, if these fluid collections exert pressure on the brain and cause symptoms or accelerated head growth, surgical treatment may be required.
Ventriculomegaly is a condition when the fluid chambers in the brain are larger than average. In many cases, Ventriculomegaly (large fluid chambers) is an isolated condition, unlinked to other health problems and will resolve on its own.
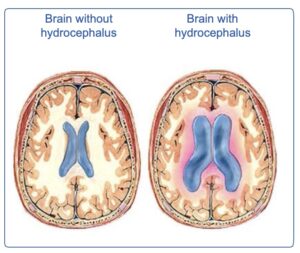
However, sometimes your child’s ventricles can get too large and put pressure on your child’s brain. This is called hydrocephalus and if not treated can cause problems.
There are many causes of hydrocephalus. Sometimes however, the cause is unknown. Hydrocephalus may present when a child is born but is not usually inherited from a parent. It may also happen as a result of other conditions such as:
- Prematurity – Hydrocephalus can occur as a complication of being born too early, and when there has been some bleeding in the brain.
- Spina Bifida – Children with spina bifida often develop hydrocephalus
- Meningitis – Hydrocephalus can occur as a complication of meningitis as the infection may cause a problem with reabsorption of the CSF.
- Tumours or Cysts – Some children with brain tumours may develop hydrocephalus as the tumour may interrupt the flow of CSF.
- Head Injury – Some children may develop hydrocephalus after having a head injury.
- Some Syndromes
For under the age of 1 year old
- Enlargement of their head (getting larger)
- The fontanelle (soft spot on top of head) may become full and hard.
- Your baby may vomit or refuse feeds
- Your child may sleep more
- Irritability-more difficult to settle/comfort
- Downward looking eyes (Cannot look upwards)
- May have a high pitched cry
- Seizures / fits
For toddlers and older children:
- Enlargement / head getting larger
- Headache orvomiting
- Dizziness
- Seizures / fits weakness in legs or arms.
- Drowsiness / sleeping a lot
- Irritability / change in personality
- Visual (eye) problems / Sensitivity to lights
- Loss of previous ability- for example weakness in legs or arms.
Your child will have signs and symptoms of hydrocephalus. Your doctor may need to do a CT scan and maybe also a MRI scan to have a closer look at your child’s fluid chambers in the brain.
- Head circumference measurement can show any excessive or limited growth.
- The size of your child’s skull reflects the growth of their brain. So if a baby’s brain isn’t growing and developing normally, their head circumference may not be increasing as it should. On the other hand, if their skull grows too quickly, it could be a sign of a problem like hydrocephalus (the build-up of fluid inthe brain). Both conditions are unlikely, but important to rule out.
- Babies heads are disproportionately large compared to adult’s heads, so don’t worry if your baby’s head looks big to you. Consider your own proportions. If you or your partner has a large or small head, your baby might too.
- By plotting your child’s head circumference on the centile chart we can track what the rate of growth is and it can help us detect if there are any increases in head circumference measurements, which may indicate an increase in fluid.
If your child develops hydrocephalus, they will need an
operation to relieve the pressure caused by a build-up of fluid (CSF). This fluid can be drained in various different ways.
Ventricular Access Device
A Ventricular Access Device (VAD) is sometimes inserted in babies to allow drainage of fluid (CSF). They are inserted usually in babies that are not quite big enough for shunts. They may also be used for babies that have some blood in their fluid chambers. Once the babies reach an optimum weight and once the blood is cleared from the fluid chambers, the baby can then proceed to have a shunt inserted if it is required.
Ventriculoperitioneal (VP) Shunt
A shunt is a tube which is inserted into the fluid chambers (ventricles) and is passed down into the lining of the child’s tummy. It allows the excess fluid from the ventricles to drain, preventing it from building up in the child’s brain causing symptoms. Inside the shunt there is a valve that controls the flow of the CSF.
There are two different types of shunts – a). fixed pressure b) programmable.
Once your child’s shunt is inserted, the neurosurgery doctor or nurse will inform you which one was inserted and they will give you documentation (shunt alert card) detailing all the information about the shunt. It is important that you keep this card safe and bring it with you to all hospital appointments.
Ventriculoatrial (VA) shunt
Sometimes if there are issues with the tummy absorbing this fluid, the neurosurgeon may decide to put the shunt in the heart. This shunt will be placed in the ventricles ( fluid chambers) of the brain and passed down to the right atrium of the heart instead of the abdomen.
Endoscopic Third Ventriculostomy ( ETV)
This operation involves the neurosurgeon making a small hole in the third ventricle in the brain to allow the fluid (CSF) to drain. Not all children may be suitable for this type of operation so your consultant will discuss this with you and your child. An MRI scan will probably be performed prior to this surgery.
The child will be discharged once they are comfortable, eating and drinking and mobilising around the ward. This can be quite quickly post shunt and ETV. For some children, they may be discharged after 1-2 days and for others it may take a few days longer to adjust to having a shunt inserted or an ETV performed. If it is the child’s first shunt, they will have two wounds (one on their head and one on their tummy). Advice will be given by the neurosurgical team how to care for these wounds and they will be checked at the follow up out-patients appointment. For the majority of children, they will have dissolvable sutures inserted. Once discharged from hospital, an appointment will be made for you to return to the Neurosurgery Advanced Nurse Practitioner (ANP) clinic for 4-6 weeks.